Your Account
2024 © D'vakaso.
Designed by Zeptt Technologies
Designed by Zeptt Technologies
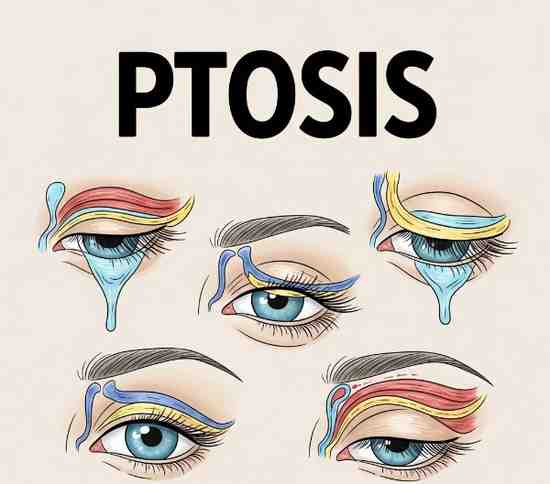
Ptosis is defined as the drooping of the upper eyelid due to dysfunction of the muscles that elevate the eyelid. In Ayurveda, it is correlated with "Vartma Patana" or "Akshi Vartma Vikara" based on symptom similarity.
ETYMOLOGY AND DEFINITION
Ptosis comes from the Greek word “πτῶσις” meaning “falling.”
It refers to a drooping of the upper eyelid, which may be unilateral or bilateral.
Ptosis can be congenital or acquired.
ETIOLOGY (NIDANA)
A. ACCORDING TO AYURVEDA
Vata Vyadhi: Ptosis is often considered a Vata-dominant disorder.
Excessive ruksha (dry), sheeta (cold), and laghu (light) ahara-vihara lead to vata prakopa.
Abhighata (trauma) to the eye or eyelid region.
Shira abhighata (head injury) can cause cranial nerve palsy affecting eyelid movement.
Dhatukshaya, especially of mamsa dhatu (muscle tissue) and majja dhatu (nervous tissue).
Avarana (obstruction) of vata by kapha or pitta.
Sanskrit Reference:
“वायुर्विदारणात् कुर्यात् नेत्रस्य चलनं तथा ।
वर्तनं पतति भ्रान्तं संकुचत्यथवा स्थिरम् ॥”
– Ashtanga Hridaya Uttara Tantra, 13/8
(Explains vata involvement leading to abnormal eye movements and eyelid dysfunction)
B. ACCORDING TO MODERN MEDICINE
Congenital Causes:
Congenital myogenic ptosis (levator muscle dystrophy)
Congenital neurogenic (third nerve palsy, Horner’s syndrome)
Acquired Causes:
Neurogenic: Third nerve palsy, Horner’s syndrome, Myasthenia gravis
Myogenic: Myopathy, muscular dystrophy
Aponeurotic: Senile or involutional ptosis due to disinsertion or dehiscence of levator aponeurosis
Mechanical: Tumor, edema, or scarring pulling down eyelid
Traumatic: Injury to nerve or muscle involved in eyelid elevation
CLINICAL FEATURES (LAKSHANA)
A. AYURVEDIC FEATURES
Vartma patana (eyelid drooping)
Aakunchana (inability to lift eyelid properly)
Sthirata (stiffness or immobility of eyelid)
Netra daurbalya (eye fatigue or weakness)
Associated features may include shiro ruk (headache), akshi ruk (eye pain) due to vata prakopa.
B. MODERN FEATURES
Drooping of upper eyelid (partial or complete)
Visual field obstruction
Chin elevation (compensatory head posture)
Eyebrow elevation (frontalis overaction)
Fatigability (seen in myasthenia gravis)
Unequal palpebral fissure height
Anisocoria (unequal pupil size) in Horner’s syndrome
Diplopia (double vision) in neurogenic causes
PRINCIPLE OF TREATMENT (CHIKITSA SIDDHANTA)
A. AYURVEDIC MANAGEMENT
Chikitsa Sutra: Vata Anulomana, Balya, Brimhana, Snehana, and Nadi Sweda
SNEHANA (OLEATION)
Abhyanga with medicated oils like Mahamasha taila, Ksheerabala taila
Helps in reducing vata and improving muscle tone
SWEDANA (SUDATION)
Nadi sweda over eye and periocular muscles
Improves local circulation and neuromuscular response
NASYA KARMA
Use of anu taila, shadbindu taila as nasal drops
Especially beneficial in urdhwajatrugata vata rogas
SHIROBASTI / SHIRODHARA
With Bala taila, Brahmi taila
Strengthens cranial nerves and improves neurological function
NETRA TARPANA / PUTAPAKA
Using ghee preparations to nourish eye muscles
Triphaladi ghrita, Jeevantyadi ghrita used
ORAL MEDICINES
Ashwagandha, Brahmi, Vacha, Rasna, Shankhapushpi, Suvarna bhasma, Mahayogaraj Guggulu
For vata shamanam and nervine strengthening
Sanskrit Reference:
"तत्र स्नेहस्वेदनाभ्यङ्गनस्यादीनि च कारयेत्।
नस्यं नेत्रतरं चैव, स्वेदादीनि प्रयोजयेत्॥"
– Ashtanga Hridaya Uttara Tantra, 13/17
B. MODERN TREATMENT
1. IDENTIFICATION AND TREATMENT OF UNDERLYING CAUSE
Myasthenia gravis: anticholinesterase drugs (e.g. pyridostigmine), corticosteroids
Third nerve palsy: investigation for aneurysm, diabetes control
Horner’s syndrome: treat underlying pathology
2. SURGICAL MANAGEMENT
Frontalis sling surgery – for severe ptosis with poor levator function
Levator resection – for moderate ptosis with fair levator function
Müller’s muscle-conjunctival resection – for mild ptosis with good levator function
3. NON-SURGICAL OPTIONS
Ptosis crutch – mechanical support in spectacle frames
Physiotherapy – in neurogenic or traumatic ptosis (limited role)
PROGNOSIS (SADHYASADHYATA)
Ayurveda: Prognosis depends on dosha predominance, chronicity, and dhatu involvement. Early stages with vatika predominance respond well.
Modern medicine:
Congenital ptosis: surgical correction often needed
Myasthenia gravis-related: variable prognosis depending on systemic control
Third nerve palsy: may recover partially or fully over time